 Suche
Suche
 Mein Konto
Mein Konto
Bladder exstrophy
Bladder exstrophy
overview
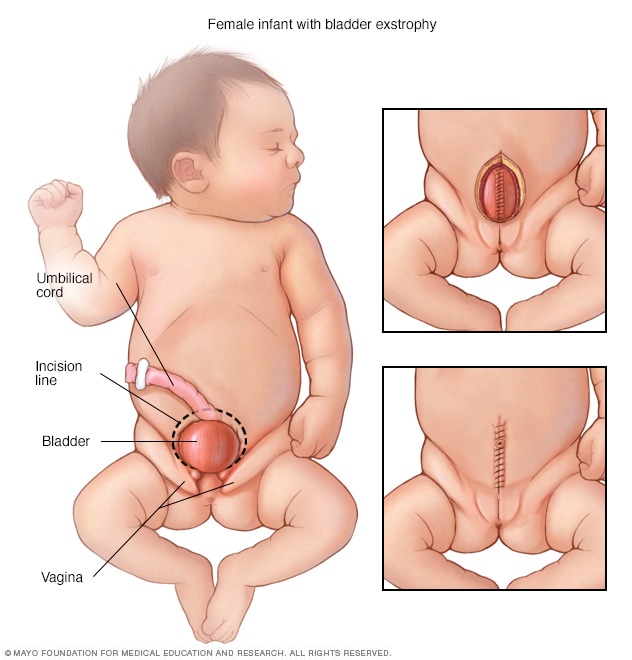
Bladder exstrophy in a female infant
Bladder exstrophy in a female infant
In girls born with bladder exstrophy, the bladder is outside the body and the vagina is not fully formed. Surgeons close the bladder (top right) and then close the abdomen and skin (bottom right).
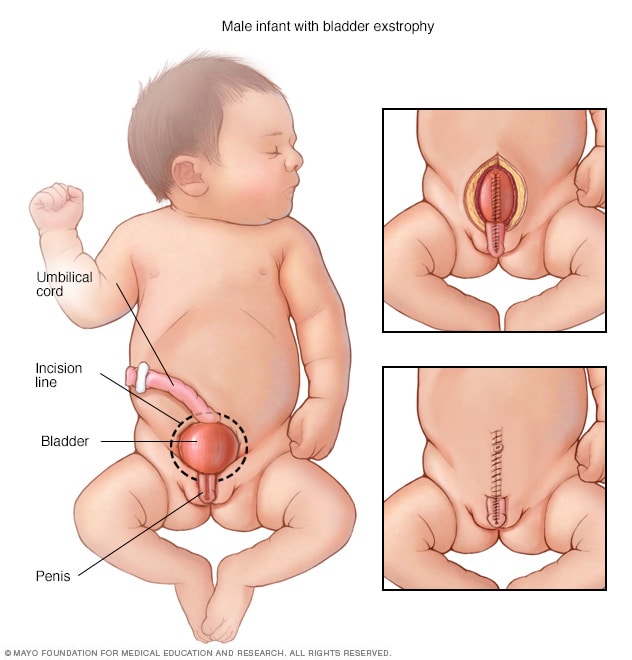
Bladder exstrophy in a male infant
Bladder exstrophy in a male infant
In boys born with bladder exstrophy, the bladder is outside the body and the penis and urethra (urethra) are not completely closed. Surgeons close the penis and bladder (top right) and then close the abdomen and skin (bottom right).
Bladder exstrophy (EK-stroh-fee) is a rare birth defect in which the bladder develops outside the fetus. The exposed bladder cannot store urine or function normally, resulting in urine leakage (incontinence).
Problems caused by bladder exstrophy vary in severity. They can include defects of the bladder, genitals and pelvic bones, as well as defects of the intestines and reproductive organs.
Bladder exstrophy can be discovered during a routine ultrasound during pregnancy. However, sometimes the defect is not visible until after the baby is born. Babies born with bladder exstrophy require surgery to correct the defects.
Symptoms
Bladder exstrophy is the most common in the larger group of birth defects called bladder exstrophy-epispadias complex (BEEC). Children with BEEC have any of the following:
- Epispadie. Dies ist die am wenigsten schwere Form von BEEC, bei der sich die Harnröhre (Harnröhre) nicht vollständig entwickelt.
-
Bladder exstrophy.This defect causes the blister to form on the outside of the body. The bladder is also inverted. Typically, bladder exstrophy affects organs of the urinary tract and digestive and reproductive systems. Defects of the abdominal wall, bladder, genitals, pelvic bones, end of the large intestine (rectum), and the opening at the end of the rectum (anus) may occur.
Children with bladder exstrophy also have vesicoureteral reflux. This condition causes urine to flow in the wrong direction - from the bladder back into the tubes connected to the kidneys (ureters). Children with bladder exstrophy also have epispadias.
-
cloacal exstrophy.Cloacal exstrophy (kloe-A-kul EK-stroh-fee) is the most severe form of BEEC. In this condition, the rectum, bladder, and genitals do not completely separate as the fetus develops. These organs may not be formed properly, and the pelvic bones are also affected.
The kidneys, spine and spinal cord may also be affected. Most children with cloacal exstrophy have spinal abnormalities, including spina bifida. Children born with protruding abdominal organs are also likely to have cloacal exstrophy or bladder exstrophy.
Causes
The cause of bladder exstrophy is unknown. Researchers believe a combination of genetic and environmental factors likely play a role.
What is known is that as the fetus grows, a structure called the cloaca (klo-A-kuh) - where the reproductive, urinary and digestive openings come together - does not develop properly in babies who develop bladder exstrophy. Defects in the cloaca can vary greatly depending on the age of the fetus when the developmental defect occurs.
Risk factors
Factors that increase the risk of bladder exstrophy include:
- Familiengeschichte. Erstgeborene Kinder, Kinder eines Elternteils mit Blasenekstrophie oder Geschwister eines Kindes mit Blasenekstrophie haben eine erhöhte Chance, mit dieser Erkrankung geboren zu werden.
- Wettrennen. Blasenekstrophie ist bei Weißen häufiger als bei anderen Rassen.
- Sex. Mehr Jungen als Mädchen werden mit Blasenexstrophie geboren.
- Einsatz der assistierten Reproduktion. Kinder, die durch assistierte Reproduktionstechnologie wie IVF geboren wurden, haben ein höheres Risiko für Blasenekstrophie.
Complications
Without surgery
Without treatment, children with bladder exstrophy cannot hold urine (urinary incontinence). They are also at risk for sexual dysfunction and have an increased risk of bladder cancer.
After the operation
Surgery can reduce complications. The success of the operation depends on how severe the defect is. Many children who undergo surgery are able to retain urine. Young children with bladder exstrophy may walk with their legs turned slightly outward due to the separation of their pelvic bones.
Long-term complications
People born with bladder exstrophy can continue to have normal sexual function, including the ability to have children. However, pregnancy poses a high risk to both mother and baby, and a planned cesarean delivery may be necessary.
Treatment of bladder exstrophy
Sources:
- Kliegman RM, et al., Hrsg. Anomalien der Blase. In: Nelson Lehrbuch der Kinderheilkunde. 21. Aufl. Elsevier; 2020. https://www.clinicalkey.com. Abgerufen am 7. November 2019.
- Was ist Blasenekstrophie? Urologische Pflegestiftung. https://www.urologyhealth.org/urological-conditions/bladder-exstrophy. Abgerufen am 4. November 2019.
- Bohrer JG. Klinische Manifestationen und anfängliches Management von Säuglingen mit Blasenexstrophie. https://www.uptodate.com/contents/search. Abgerufen am 8. November 2019.
- Ellison JS, et al. Eine kritische Bewertung der Kontinenz bei Blasenekstrophie: Langzeitergebnisse der vollständigen primären Reparatur. Zeitschrift für Kinderurologie. 2016; doi:10.1016/j.jpurol.2016.04.005.
- Bohrer JG. Chirurgisches Management und postoperatives Ergebnis von Kindern mit Blasenexstrophie. https://www.uptodate.com/contents/search. Abgerufen am 8. November 2019.
- Coran AG, et al., Hrsg. Blasen- und Kloakenekstrophie. In: Kinderchirurgie. 7. Aufl. Elsevier; 2012. https://www.clinicalkey.com. Abgerufen am 7. November 2019.
- Szymanski KM, et al. Wahrscheinlichkeit einer Blasenaugmentation, -umleitung und sauberen intermittierenden Katheterisierung bei klassischer Blasenexstrophie: Eine 36-jährige, multiinstitutionelle, retrospektive Kohortenstudie. Das Journal der Urologie. 2019; doi:10.1097/JU.0000000000000552.
- Cote C, et al., Hrsg. Allgemeine abdominale und urologische Chirurgie. In: Anästhesiepraxis für Säuglinge und Kinder. 6. Aufl. Elsevier; 2019. https://www.clinicalkey.com. Abgerufen am 7. November 2019.
- Wein AJ, et al., Hrsg. Exstrophie-Epispadie-Komplex. In: Campbell-Walsh-Urologie. 11. Aufl. Elsevier; 2016. https://www.clinicalkey.com. Abgerufen am 7. November 2019.
- Gargollo PC, et al. Komplexe robotische Operation der unteren Harnwege bei Patienten mit offener Operation in der Vorgeschichte. Das Journal der Urologie. 2019; doi:10.1016/j.juro.2018.06.017
- Husmann DA. Lehren aus der Behandlung von Erwachsenen, die sich einer Augmentation wegen Spina bifida und Blasenexstrophie unterzogen haben: Inzidenz und Behandlung der nicht tödlichen Komplikationen der Blasenaugmentation. Internationale Zeitschrift für Urologie. 2018; doi:10.1111/iju.13417
- Braswell-Pickering EA. Allscripts EPSi. Mayo-Klinik. 8. Juli 2021.