 Suche
Suche
 Mein Konto
Mein Konto
Uterine fibroids
Uterine fibroids
overview
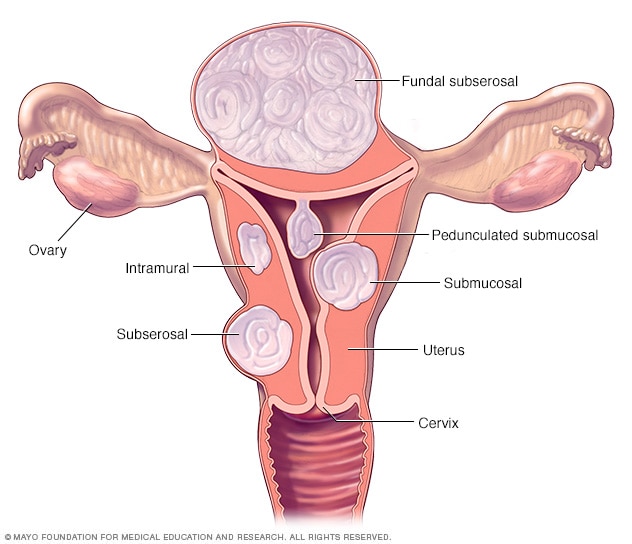
Localization of fibroids
Localization of fibroids
There are three main types of uterine fibroids. Intramural fibroids grow within the muscular wall of the uterus. Submucosal fibroids bulge into the uterine cavity. Subserosal fibroids protrude from the uterus. Some submucosal or subserosal fibroids may be pedunculated—hanging from a stalk inside or outside the uterus.
Uterine fibroids are benign growths of the uterus that often occur during childbearing years. Uterine fibroids, also called leiomyomas (Lie-o-my-O-muhs) or fibroids, are not associated with an increased risk of uterine cancer and almost never develop into cancer.
Fibroids range in size from seedlings that are invisible to the human eye to bulky masses that can distort and enlarge the uterus. You may have a single fibroid or multiple. In extreme cases, multiple fibroids can expand the uterus so much that they can reach the ribcage and add weight.
Many women have uterine fibroids at some point in their lives. But you may not know you have uterine fibroids because they often don't cause any symptoms. Your doctor may discover fibroids accidentally during a pelvic exam or prenatal ultrasound.
Symptoms
Many women with fibroids have no symptoms. For those who do, symptoms may be influenced by the location, size, and number of the fibroids.
In women who have symptoms, the most common signs and symptoms of uterine fibroids include:
- Starke Menstruationsblutung
- Menstruationsperioden, die länger als eine Woche dauern
- Beckendruck oder Schmerzen
- Häufiges Wasserlassen
- Schwierigkeiten beim Entleeren der Blase
- Verstopfung
- Rücken- oder Beinschmerzen
Rarely, a fibroid can cause acute pain as it outgrows its blood supply and begins to die.
Fibroids are generally classified based on their location. Intramural fibroids grow within the muscular wall of the uterus. Submucosal fibroids bulge into the uterine cavity. Subserosal fibroids protrude from the uterus.
When to go to the doctor?
See your doctor if you:
- Beckenschmerzen, die nicht weggehen
- Übermäßig schwere, verlängerte oder schmerzhafte Perioden
- Schmierblutungen oder Blutungen zwischen den Perioden
- Schwierigkeiten beim Entleeren der Blase
- Unerklärliche niedrige Anzahl roter Blutkörperchen (Anämie)
Seek immediate medical attention if you suddenly experience heavy vaginal bleeding or severe pelvic pain.
Causes
Doctors don't know the cause of uterine fibroids, but research and clinical experience point to these factors:
- Genetische Veränderungen. Viele Myome enthalten Veränderungen in Genen, die sich von denen in typischen Gebärmuttermuskelzellen unterscheiden.
-
Hormones.Estrogen and progesterone, two hormones that stimulate the development of the uterine lining during each menstrual cycle in preparation for pregnancy, appear to promote the growth of fibroids.
Fibroids contain more estrogen and progesterone receptors than typical uterine muscle cells. Fibroids tend to shrink after menopause due to a decrease in hormone production.
- Andere Wachstumsfaktoren. Substanzen, die dem Körper helfen, Gewebe zu erhalten, wie z. B. insulinähnlicher Wachstumsfaktor, können das Wachstum von Myomen beeinflussen.
- Extrazelluläre Matrix (ECM). ECM ist das Material, das Zellen wie Mörtel zwischen Ziegeln zusammenkleben lässt. ECM ist bei Myomen erhöht und macht sie faserig. ECM speichert auch Wachstumsfaktoren und verursacht biologische Veränderungen in den Zellen selbst.
Doctors believe that uterine fibroids develop from a stem cell in the smooth muscle of the uterus (myometrium). A single cell divides repeatedly, eventually forming a solid, rubbery mass that is distinct from neighboring tissue.
The growth patterns of uterine fibroids vary – they may grow slowly or quickly, or they may remain the same size. Some fibroids go through growth spurts, while others may shrink on their own.
Many fibroids that were present during pregnancy shrink or disappear after pregnancy as the uterus returns to its normal size.
Risk factors
There are few known risk factors for uterine fibroids, other than being a woman of childbearing age. Factors that can have an impact on the development of fibroids include:
- Wettrennen. Obwohl alle Frauen im gebärfähigen Alter Myome entwickeln können, haben schwarze Frauen mit größerer Wahrscheinlichkeit Myome als Frauen anderer Rassengruppen. Darüber hinaus haben schwarze Frauen Myome in jüngeren Jahren, und sie haben wahrscheinlich auch mehr oder größere Myome, zusammen mit schwereren Symptomen.
- Vererbung. Wenn Ihre Mutter oder Schwester Myome hatte, haben Sie ein erhöhtes Risiko, sie zu entwickeln.
- Andere Faktoren. Beginnen Sie Ihre Periode in einem frühen Alter; Fettleibigkeit; ein Vitamin-D-Mangel; eine Ernährung mit mehr rotem Fleisch und weniger grünem Gemüse, Obst und Milchprodukten; und Alkoholkonsum, einschließlich Bier, scheinen Ihr Risiko für die Entwicklung von Myomen zu erhöhen.
Complications
Although uterine fibroids are not usually dangerous, they can cause discomfort and lead to complications such as a drop in red blood cells (anemia), which leads to fatigue due to severe blood loss. Rarely, a transfusion is required due to blood loss.
Pregnancy and fibroids
Fibroids usually do not affect pregnancy. However, it is possible that fibroids - particularly submucosal fibroids - can lead to infertility or miscarriage.
Fibroids can also increase the risk of certain pregnancy complications, such as: B. Placental abruption, fetal growth restriction and preterm birth.
prevention
Although researchers continue to study the causes of fibroids, there is little scientific evidence on how to prevent them. Preventing uterine fibroids may not be possible, but only a small percentage of these tumors require treatment.
However, if you choose a healthy lifestyle, e.g. For example, maintaining a healthy weight and eating fruits and vegetables may help reduce your risk of fibroids.
Some research also suggests that use of hormonal contraceptives may be associated with a lower risk of fibroids.
Treatment of uterine fibroids
Sources:
- Ferri FF. Uterusmyome. In: Ferri’s Clinical Advisor 2019. Philadelphia, Pa.: Elsevier; 2019. https://www.clinicalkey.com. Abgerufen am 24. April 2019.
- Stellungnahme Nr. 770 des ACOG-Ausschusses: Uterusmorcellation bei mutmaßlichen Leiomyomen. Das American College of Geburtshelfer und Gynäkologen. https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Uterine-Morcellation-for-Presumed-Leiomyomas. Abgerufen am 24. April 2019.
- Stewart EA, et al. Uterus-Leiomyome (Myome): Epidemiologie, klinische Merkmale, Diagnose und Naturgeschichte. https://www.uptodate.com/contents/search. Abgerufen am 24. April 2019.
- Farris M. et al. Uterusmyome: Ein Update zu aktuellen und neuen medizinischen Behandlungsmöglichkeiten. Therapeutik und klinisches Risikomanagement. 2019;15:157.
- Hoffman BL, et al. Beckenmasse. In: Williams Gynäkologie. 3. Aufl. New York, NY: McGraw-Hill-Bildung; 2016. https://accessmedicine.mhmedical.com. Abgerufen am 24. April 2019.
- Papadakis MA, et al., Hrsg. Gynäkologische Erkrankungen. In: Aktuelle medizinische Diagnose & Behandlung 2019. 58. Aufl. New York, NY: McGraw-Hill-Bildung; 2019. https://accessmedicine.mhmedical.com. Abgerufen am 24. April 2019.
- Stewart EA. Überblick über die Behandlung von Uterusleiomyomen (Myomen). https://www.uptodate.com/contents/search. Abgerufen am 24. April 2019.
- Hartmann KE, et al. Behandlung von Uterusmyomen. Vergleichende Wirksamkeitsprüfung Nr. 195. Agentur für Gesundheitsforschung und -qualität. https://effektivehealthcare.ahrq.gov/topics/uterine-fibroids/research-2017. Abgerufen am 24. April 2019.
- De La Cruz MS, et al. Uterusmyome: Diagnose und Behandlung. Amerikanischer Hausarzt. 2017;95:100.
- Schmied RP. Uterusleiomyome (Myome, Myome). In: Netter’s Geburtshilfe und Gynäkologie. 3. Aufl. Philadelphia, Pennsylvania: Elsevier; 2018. https://www.clinicalkey.com. Abgerufen am 24. April 2019.
- Jameson JL, et al., Hrsg. Uterusmyome. In: Endokrinologie: Erwachsene und Kinder. 7. Aufl. Philadelphia, Pennsylvania: Saunders Elsevier; 2016. https://www.clinicalkey.com. Abgerufen am 24. April 2019.
- Cheung VYT. Hochintensive fokussierte Ultraschalltherapie. Best Practice und Forschung. Klinische Geburtshilfe und Gynäkologie. 2018;46:74.
- Parker WH. Abdominale Myomektomie. https://www.uptodate.com/contents/search. Abgerufen am 1. Mai 2019.
- Kellermann RD, et al. Uterus-Leiomyome. In: Conn’s Current Therapy 2019. Philadelphia, Pa.: Elsevier; 2019. https://www.clinicalkey.com. Abgerufen am 24. April 2019.
- Uterusmyome. American College of Geburtshelfer und Gynäkologen. https://www.acog.org/Patients/FAQs/Uterine-Fibroids. Abgerufen am 2. Mai 2019.
- Kaunitz AM. Behandlung abnormaler Uterusblutungen. https://www.uptodate.com/contents/search. Abgerufen am 3. Mai 2019.
- Laparoskopische Power-Morcellatoren. Lebensmittel- und Arzneimittelverwaltung. https://www.fda.gov/medical-devices/surgery-devices/laparoscope-power-morcellators. Abgerufen am 3. Mai 2019.
- Lonnerfors C. Roboterassistierte Myomektomie. Best Practice und Forschung: Klinische Geburtshilfe und Gynäkologie. 2018;46:113.
- Fragen Sie MayoExpert. Uterusmyome. Rochester, Minnesota: Mayo Foundation for Medical Education and Research; 2018.
- Jarell JF, et al. Nr. 164 – Konsensrichtlinien für die Behandlung chronischer Unterbauchschmerzen. Zeitschrift für Geburtshilfe und Gynäkologie Kanada. 2018;40:e747.
- Warner KJ. Allscripts EPSi. Mayo Clinic, Rochester, Minnesota, 2. Mai 2019.
- Stewart EA (Expertenmeinung). Mayo Clinic, Rochester, Minnesota, 23. Mai 2019.
- Stewart EA. Klinische Praxis. Uterusmyome. New England Journal of Medicine. 2015;372:1646.
- Laughlin-Tommaso SK (Gutachten). Mayo Clinic, Rochester, Minnesota, 29. Mai 2019.
- Laughlin-Tommaso SK. Alternativen zur Hysterektomie: Behandlung von Uterusmyomen. Kliniken für Geburtshilfe und Gynäkologie in Nordamerika. 2016;43:397.